Child with a cough X-ray
Date: 2026-04-24
Accepted answers: Viral Lower Respiratory Tract Infection
Explanation
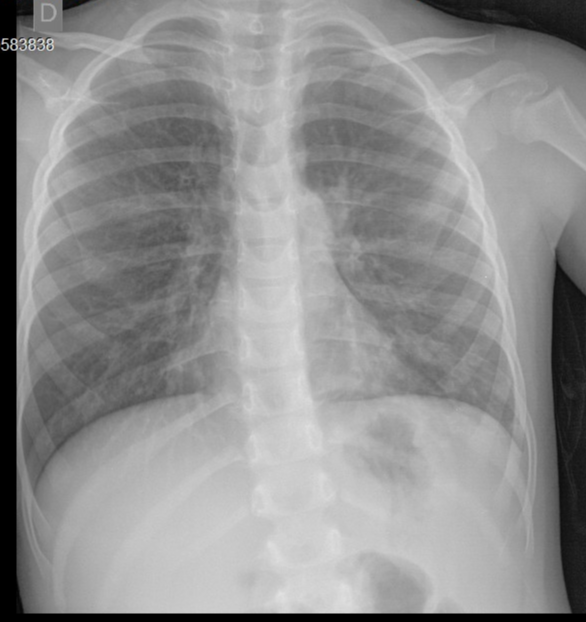
The chest radiograph demonstrates bilateral perihilar peribronchial thickening, interstitial opacities, and ring shadows representing inflamed bronchial walls seen end-on, the classic "dirty chest" appearance of viral lower respiratory tract infection. This pattern reflects diffuse airway-centered inflammation caused by viral invasion of bronchial epithelium, leading to mucosal edema and peribronchial infiltration rather than alveolar consolidation. The absence of focal lobar consolidation distinguishes this from bacterial pneumonia, while the interstitial distribution and bilateral symmetry support a viral etiology. In the clinical context of a young child with recent fever, persistent cough, and bronchodilator-responsive hypoxemia, these findings are consistent with viral bronchiolitis or reactive airways disease triggered by a respiratory virus such as RSV or rhinovirus.
Source: Giménez Chilavert J, Viral lower respiratory tract infection. Case study, Radiopaedia.org (Accessed on 23 Apr 2026) https://radiopaedia.org/cases/234267
Hints
- A 4-year-old girl is brought to clinic after three days of fever and cough. The fever has since resolved, but she has persistent cough and her oxygen saturation is 93% on room air.
- On auscultation, wheezing is not clearly appreciated despite cough and borderline oxygen saturation. After bronchodilator therapy, her oxygen saturation improves.
- Chest radiography is obtained given her borderline hypoxemia and persistent cough despite clinical improvement. Imaging demonstrates bilateral perihilar and interstitial opacities without focal lobar consolidation, pleural effusion, or pneumothorax.
- She has a known history of bronchial hyperreactivity, and her mother reports that the fever resolved three days before presentation, with the cough being the primary ongoing concern.
- Imaging shows ring opacities representing bronchial wall thickening seen, with poorly delineated bronchovascular markings. With findings that reflect airway-centered inflammation rather than alveolar filling.
- This pattern of bilateral perihilar peribronchial thickening with interstitial opacities in a young child with recent fever, cough, and bronchospastic response to bronchodilators is most consistent with the most common infectious cause of lower respiratory illness in the pediatric population.