Trouble in the scan X-ray
Date: 2026-02-14
Accepted answers: Mercury Embolism
Explanation
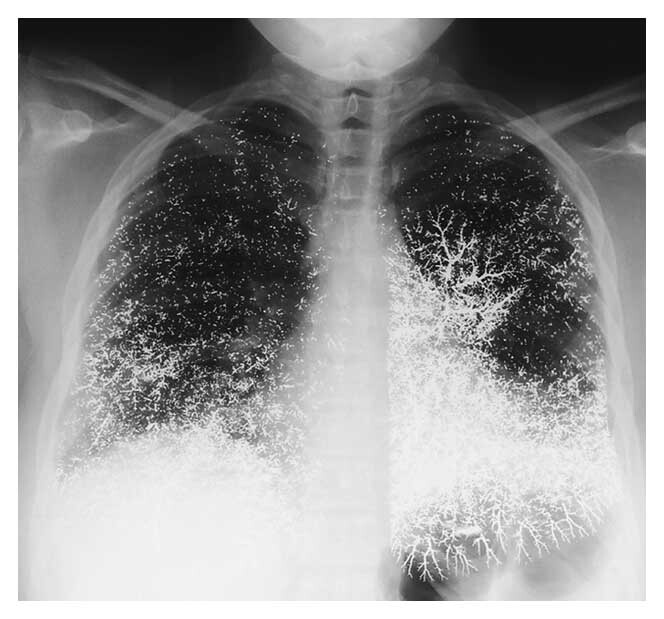
Learning case: A young patient with a history of intravenous drug use or intentional self-injection presents with acute cough, dyspnea, and occasionally hemoptysis. Chest radiograph reveals numerous bilateral, intensely radiopaque, metallic-density opacities scattered throughout both lung fields, many outlining the branching pulmonary arterial tree in a vascular pattern consistent with hematogenous spread. These findings are classic for mercury embolism following intravenous injection. Elemental mercury enters the venous circulation, travels to the pulmonary arteries, and becomes mechanically lodged in distal vessels, producing characteristic high-density droplets on imaging. Management is largely supportive, with consideration of chelation therapy in cases of systemic toxicity.
Source: https://www.nejm.org/doi/full/10.1056/NEJM200006153422405
Hints
- 21 yo F with history of depression presents to the emergency room with tachypnea, a dry cough, and bloody sputum
- lung fields contain numerous extremely bright white foci that stand out sharply against surrounding lung tissue. denser than calcified granulomas, standard contrast opacification
- findings are present bilaterally, spread throughout multiple lobes, indicating a hematogenous spread
- Opacities trace the outline of the pulmonary arterial branches to form a "tree-like" configuration. This vascular distribution strongly suggests embolization via the bloodstream.
- Many of the opacities appear as discrete, spherical droplets, which is classic for an injected liquid substance entering the bloodstream.
- Chest radiograph demonstrates numerous, bilateral, highly radiopaque metallic-density opacities distributed throughout both lung fields, many of which outline the branching pulmonary arterial tree in a vascular pattern consistent with hematogenous embolization.